All published articles of this journal are available on ScienceDirect.

The Impact of Vitiligo on Patients' Psychological Status and Sexual Function: Cross-Sectional Questionnaire-Based Study
Abstract
Introduction:
Vitiligo is a chronic pigmentary cutaneous disorder. Although vitiligo is not a life-threatening disease, it seriously affects patients' psychological status and Quality-of-Life (QoL). Moreover, the effect of vitiligo on genital image severely affects sexual function, especially in females.
Patients & Methods:
This cross-sectional questionnaire-based study had targeted patients with vitiligo of both genders. 173 patients who had responded to the given questionnaires were included and their responses were statistically analyzed. Patients’ files were revised for extraction of demographic and clinical data and the previous evaluation of the Vitiligo Area Scoring Index (VASI) score.
Results and Discussion:
Median VIS-22 score was in the range of 21-49, but 109 patients had a median score of 28. Seventy-eight patients had mild and 15 patients had moderate depression. Regression analysis defined the sense of being unattractive, disappointed in self and discouragement about the future as the most significant underlying causes of depression. Ninety-two patients had sexual dysfunction and scoring of satisfaction by the sexual act was the highest while scoring for the desire was the lowest. Regression analysis revealed that female gender, high ASEX and VASI scores are the significant predictors for high BDI-II. ROC curve analysis defined a high ASEX score as a significant predictor for a high BDI-II score.
Conclusion:
The obtained results indicated a deleterious effect of vitiligo on patients’ psychological status that may progress to depression. The effects of the disease on body image, especially the genital area, induced sexual dissatisfaction with an impact on sexual function. Altogether, raise a suggested adjuvant role for psychotherapy in patients with vitiligo which might even indirectly lead to improvement of vitiligo.
1. INTRODUCTION
Vitiligo is a common chronic autoimmune disease characterized by progressive loss of skin color due to melanocyte destruction [1]. It is an acquired skin disease with unclear, multifactorial etiopathogenesis, which is also associated with metabolic abnormalities, confirming the systemic nature of the disease [2]. Cellular oxidative stress secondary to increased release of reactive oxygen species was implicated in the pathogenesis of vitiligo through downregulation of nuclear factor E2-related factor 2/ antioxidant response element pathway, which plays an important role in melanocytes against hydrogen peroxide-induced oxidative stress [3]. As another possible pathogenesis, immune pathogenesis of vitiligo was supposed and so it was considered as chronic autoimmune skin disease leads to the loss of epidermal melanocytes [4].
Vitiligo seriously affects patients’ physical and mental health and their quality of life [5]. Adverse psychological effects induced by this depigmented disease cause social stigmatization and patients who are employed or have new lesions are significantly more vulnerable to be depressed [1]. Moreover, the partial response to therapy and long duration required for re-pigmentation augment the psychological impact of the disease and obligate the patients to shift to the camouflaging technique through concealing vitiligo lesions to improve their confidence and self-esteem [6].
Vitiligo has a major effect on sexual health because of the disfiguring skin lesions which affect self-image, self-esteem [7] an individual's emotional and psychological well-being and relationships with other people [8]. Genital self-image is an emerging aspect of body image relevant to sexual functioning and sexual satisfaction [9]. Women are the most dissatisfied with their body image especially if associated with disfigured genital-image secondary to extension of depigmentation to the genital region [10].
The current study aimed to evaluate the impact of vitiligo on patients' Quality of Life (QoL), psychological status, and sexual function using the online Arabic version of Vitiligo Impact Scale-22, Beck Depression Inventory-II, and Arizona Sexual Experiences Scale questionnaires.
2. MATERIALS AND METHODS
2.1. Study Design
This cross-sectional self-assessment online questionnaire-based study was conducted from Aug 2019 to Sep 2020, at The Department of Dermatology, Faculty of Medicine, Qassim University, Saudi Arabia, in conjunction, using online communication, with The Department of Dermatology, Faculty of Medicine, Benha University, Egypt
2.2. Study Plan
The study protocol was approved by the Research Ethics Committee at The Faculty of Medicine, Benha University on 15-7-2019; No. 0044. At the registry of Dermatology Department, Benha University Hospital, the files of all patients with vitiligo were revised. Patients with severe psychiatric or systemic illnesses were excluded from the study. Inclusion criteria include patients older than 20 years of both genders and with clinically established diagnoses of vitiligo.
Demographic and general clinical data of patients who were free of exclusion criteria were extracted and collected. The enrolled files include the previous estimation of the Vitiligo Area Scoring Index (VASI) score, which is determined by calculating the affected surface area of vitiligous skin as obtained by the sum of Hand-Units of all body sites multiplied by the extent of residual depigmentation for a possible range of 0–100 [11].
Then, the enrolled patients were communicated to discuss the objectives and methodology of the current study. After that, the study questionnaires were sent to those who had accepted to participate in the study and the responses of these patients were analyzed. Filling the questionnaire sheets was considered as an approval to join the study.
2.3. Tools
2.3.1. Vitiligo Impact Scale (VIS)-22 [12].
The VIS-22 is a vitiligo-specific quality-of-life self-report instrument consisted of 22-items, each item scoring on a 4-point scale (0-3) with a total score ranged between 0 and 66. Recently, Gupta et al. [13] documented that VIS-22 is comparable to Dermatology Life Quality Index and Skindex-16 questionnaires for being a valid, reliable and responsive QoL instrument, and is specific to the needs of patients with vitiligo.
2.3.2. Beck Depression Inventory-II (BDI-II) [14]
The BDI-II is a self-report instrument designed to assess the severity of current depressive symptoms within the last 2 weeks in adolescents and adults. It is a 21-items instrument in which each item is rated on a 4-point scale (0–3) with total scores ranging from 0 to 63. According to Poole et al. [15], a cut-off of 22 for discrimination of depression provided 89% sensitivity and 90% specificity and BDI-II score ranged between 22-32 was considered as mild, 33-44 was considered as moderate and >44 was considered as severe depression.
2.3.3. Arizona Sexual Experiences Scale (ASEX) [16]
The ASEX is a 5-item questionnaire used in clinical trials to assess sexual functioning. Each item is scored from 1 to 6, for a total score is from 5 to 30. Sexual dysfunction is defined as a total ≥19 or ≥5 for any item, or ≥4 on three items.
3. METHODS
The three questionnaires were translated into Arabic language to be self-administered by the patients. They were prepared as online questionnaires and uploaded on Google forms at the following links to allow self-administration without direct contact with the dermatologist:
- https://forms.gle/qmHqYfMJrM6jUZvS6
- https://forms.gle/YESaL3mSMYKgxgjb6
- https://forms.gle/K7zLEPUb2Laxf98H6
4. STATISTICAL ANALYSIS
Obtained data were presented as mean, standard deviation, numbers, percentages, median and interquartile range. Age, gender, Body Mass Index (BMI), educational levels, vitiligo disease type, duration, severity, response to therapy and VASI score as a judge for disease extent and severity were evaluated as predictors for the development of depression as judged by BDI-II score, impact on sexual function as judged by ASEX score using the Regression analysis (Stepwise method) and the Receiver Operating Characteristic (ROC) curve analysis judged by the Area Under the Curve (AUC) compared versus the null hypothesis AUC=0.05. Statistical analysis was conducted using the SPSS (Version 26, 2015) for Windows using a password-protected Laptop. P-value <0.05 was considered statistically significant.
5. RESULTS
There were 269 files of vitiligous patients in the hospital registry of which 31 files were excluded for not fulfilling the inclusion criteria. Then, 238 files were revised and patients were communicated, but 26 patients refused to participate in the study. In the end, 212 patients had received the links for the online questionnaires. Unfortunately, 25 patients did not respond and 14 responders failed to complete the questionnaires. Those 39 patients were excluded, thus only 173 responses were analyzed (Fig. 1). Demographic and clinical data of the responders are shown in Table 1.
| Data | Findings | ||
| Age (days) | 20-29 | 43 (24.9%) | |
| 30-39 | 62 (35.8%) | ||
| 40-49 | 51 (29.5%) | ||
| >50 | 17 (9.8%) | ||
| Mean (±SD) | 37.2 (8.6) | ||
| Range | 20-57 | ||
| Gender | Males | 96 (55.5%) | |
| Females | 77 (44.5%) | ||
| Educational levels | Illiterate | 13 (7.5%) | |
| Primary school graduate | 57 (32.9%) | ||
| Higher school graduate | 70 (40.5%) | ||
| University graduate | 33 (19.1%) | ||
| Body mass index (kg/m2) | Average (≤24.9 kg/m2) | 3 (1.7%) | |
| Overweight (25-30 kg/m2) | 120 (69.4%) | ||
| Obese (>30-35 kg/m2) | 50 (28.9%) | ||
| Mean (±SD) | 29.4 (2.4) | ||
| Range | 24.2-34.8 | ||
| Vitiligo disease data | Type of vitiligo | Generalized | 127 (73.4%) |
| Localized | 41 (23.7%) | ||
| Segmental | 5 (2.9%) | ||
| Duration of disease (years) | 1-4 | 35 (20.2%) | |
| 5-10 | 63 (36.4%) | ||
| 10-19 | 51 (29.5%) | ||
| ≥20 | 24 (13.9%) | ||
| Mean (±SD) | 10 (7.4) | ||
| Range | 1-31 | ||
| Response to therapy | Improved | 37 (21.4%) | |
| No change | 61 (35.3%) | ||
| Slowly progressive | 52 (30%) | ||
| Rapidly progressive | 23 (13.3%) | ||
| VASI score | <5 | 111(64.3%) | |
| 5-10 | 39 (22.5%) | ||
| 11-20 | 16 (9.2%) | ||
| >20 | 7 (4%) | ||
| Mean (±SD) | 5.9 (6.6) | ||
| Range | 0.3-36.7 | ||
The response to VIS-22 was varied, 30 patients had a median score of 21 (IQR: 17.75;22), 109 patients (63%) had a median score of 28 (IQR: 26;30), 28 patients (16.2%) had a median score of 38 (IQR: 36;39) and only 6 patients (3.5%) had a median score of 49 (IQR: 46;51), and a median total score was 28 (IQR: 24;33) (Table 2).
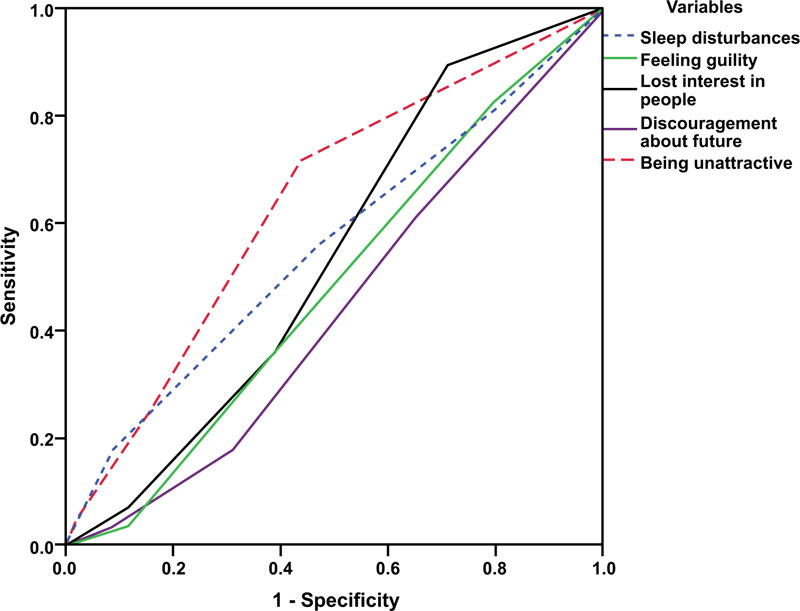
Regarding the responses to the BDI-II questionnaire, 80 patients (46.2%) had a score of <22 with a mean score and were considered free of depression. Whereas 93 patients (53.8%) had a score > 22; 78 patients (45.1%) had mild and 15 patients (8.7%) had moderate depression, but no patient had severe depression (Table 2). Regression analysis for items of BDI-II to define the most significant causative factors for inducing depression defined lost interest in people (β: 0.196, p<0.001), discouragement about future (β: 0.219, p<0.001), sleep disturbances (β: 0.221, p<0.001), disappointed in self (β: 0.273, p<0.001) and sense of being unattractive (β: 0.323, p<0.001), while ROC curve analysis defined sense of being unattractive as the most significant causative factor for the development of depression (AUC: 0.639±0.05; CI: 0.530-0.748, p=0.02) (Fig. 2).

Ninety-two patients (53.2%) had sexual dysfunction with the mean ASEX of 19 (IQR: 16.75; 24), while 81 patients (46.8%) had no evident sexual dysfunction with a median score of 11 (IQR: 8;13). The median total ASEX score for study participants was 21 (IQR: 11;21) (Table 2). Interestingly, scoring of satisfaction (4, IQR: 2-5) by the sexual act was the highest score for ASEX items, while scoring for the desire was the lowest score (2, IQR: 1-3).
Total BDI-II and VIS-22 scores of studied patients showed a negative significant correlation, while total ASEX score showed a positive significant correlation with patients’ age and duration of vitiligo. Total ASEX score also showed a positive significant correlation with patients’ BMI and disease severity as judged by VASI score, while showed a negative significant correlation with patients’ educational level and VIS-22 score. Total BDI-II score showed a negative significant correlation with male gender and patients’ ASEX score, while showed a positive significant correlation with VIS-22 score (Table 3).
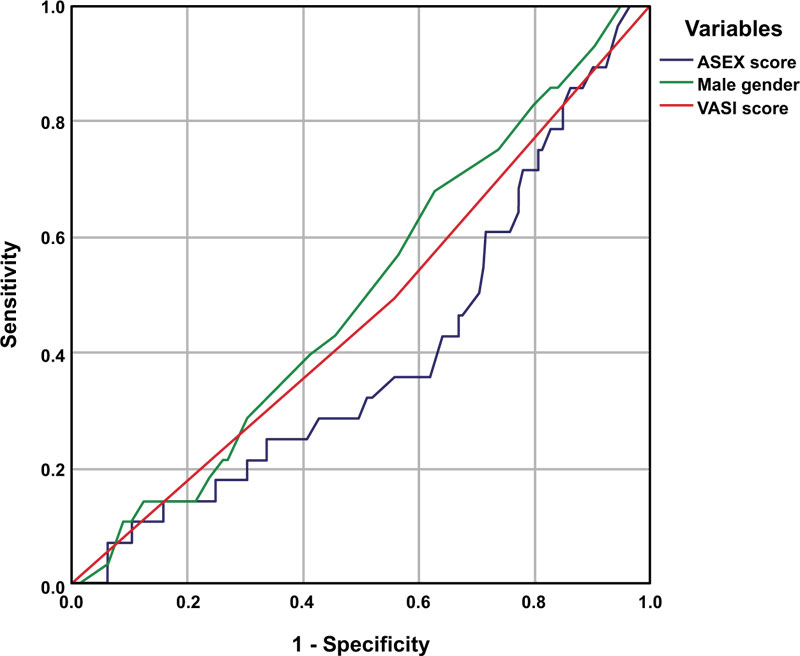
Regression analysis defined female gender (β: 0.478, p<0.001), high ASEX (β: 0.560, p<0.001), and VASI (β: 0.109, p=0.036) scores as the significant predictors for development of depression. The results also revealed that the higher ASEX and VASI scores, the higher the BDI-II score. ROC curve analysis defined a high ASEX score as the significant sensitive predictor for a high BDI-II score with AUC of 0.398 (±0.058, 95% CI: 0.285-0.512, p=0.038) (Fig. 3).
| Questionnaires | Cutoff points | Number (%) | Median (IQR) score |
| VIS-22 | ≤22 | 30 (17.3%) | 21 [17.75;22] |
| 23-33 | 109 (63%) | 28 [26;30] | |
| 34-44 | 28 (16.2%) | 38 [36;39] | |
| >44 | 6 (3.5%) | 49 [46;51] | |
| Total | 173 (100%) | 28 [24;33] | |
| BDI-II score | <22 (No depression) | 80 (46.2%) | 13.7±3 |
| 22-33 (Mild depression) | 78 (45.1%) | 25.4±3.3 | |
| 34-44 (Moderate depression) | 15 (8.7%) | 36.1±2.8 | |
| Total | 173 (100%) | 19 [16.75;24] | |
| ASEX score | No sexual dysfunction | 81 (46.8%) | 11 [8;13] |
| Sexual dysfunction | 92 (53.2%) | 19 [16.75;24] | |
| Total | 173 (100%) | 21 [16.75;24] |
| Variables | ASEX | BDI -II | VIS-22 | |||
| r | p | r | p | r | p | |
| Age | 0.762 | <0.001 | -0.308 | <0.001 | -0.778 | <0.001 |
| Male gender | 0.060 | 0.436 | -0.603 | <0.001 | -0.004 | 0.956 |
| Duration of disease | 0.610 | <0.001 | -0.195 | 0.010 | -0.575 | <0.001 |
| Education | -0.256 | 0.001 | 0.059 | 0.437 | 0.129 | 0.091 |
| BMI | 0.166 | 0.029 | -0.088 | 0.249 | -0.038 | 0.615 |
| VASI | 0.218 | 0.004 | 0.080 | 0.298 | -0.061 | 0.429 |
| ASEX | - | - | -0.488 | <0.001 | -0.572 | <0.001 |
| BDI-II | - | - | - | - | 0.337 | <0.001 |
6. DISCUSSION
Analysis of the responses to the BDI-II questionnaire detected depression of all vitiligo patients but varied. About 53.8% of patients had manifested depression with a median score of > 22, which is previously documented [15] as the cutoff point for the BDI-II questionnaire. These findings illustrated the deleterious effect of vitiligo on patients’ psychological status. In support of this assumption, there was a negative significant correlation between BDI-II and VIS-22 scores with a positive significant correlation with duration of disease. Similarly, Salman et al. [17] found that vitiligo patients had higher levels of social anxiety and depression compared with healthy control subjects. Yucel et al. [8] reported significantly higher scores in comparison to controls by using four documented scoring inventories to evaluate the psychological and sexual status of vitiligo patients.
These data indicated a reciprocal relationship between vitiligo and depression and supported as previously observed by Cunliffe & Cotterill [18], who detected exacerbation of dermatological conditions with major stressful events and mental trauma. Also, Nock et al. [19] supposed that certain dermatological symptoms may be a sign of psychiatric disorders. Thereafter, Wang et al. [20] found that patients with vitiligo were 4.96 times more likely to have Major Depressive Disorders (MDD) than controls, with a prevalence of MDD of 33% among vitiligo patients. Similarly, and in adjusted models, Vallerand et al. [21] found MDD patients were at a 64% increased risk for vitiligo.
Analysis of DBI-II item-scoring using Regression analysis defined sense of being unattractive, disappointed in self, and discouragement about future are the main depressive factors. ROC curve analysis had defined the sense of being unattractive as the most significant depressive factor, thus indicating that patients’ disappointment by their body image induced their social isolation and can be considered the main underlying factor for developing depression. In hand with these data, Bonotis et al. [22] found distorted body image secondary to vitiligous lesions negatively affects patients’ QOL and psychosocial health. The impacts of vitiligo on QOL were significantly associated with disease variables, including duration, severity, distribution, personality traits, and gender.
Evaluation of the patients’ responses to the ASEX questionnaire had defined 92 patients with sexual dysfunction. Scoring for satisfaction by the sexual act was the highest, while scoring for the desire was the lowest. A finding points to low satisfaction despite the good desire, thus indicating sexual dysfunction. Sexual dysfunction was found to be related to the severity of vitiligo disease and patients’ evaluation of disease impact on their QOL while it was negatively correlated with patients' psychological status. These findings are in line with that previously reported by Sarhan et al. [7], who found a negative correlation between VASI score and sexual satisfaction. Also, Morales-Sánchez et al. [23] reported that QOL was worse in vitiligo patients with genital lesions. Recently, Yucel et al. [8], using Golombok-Rust-Inventory-of-Sexual-Satisfaction had detected significantly lower sexual satisfaction levels among vitiligo patients in comparison to controls.
The obtained results indicated the presence of a triangle of danger, which is consisted of vitiligo disease severity, depression and sexual dysfunction. This triangle seriously impairs patients’ QOL to suicidal ideations or even attempts. This is shown by the finding that 56.6% of the study’s participants had scored suicide ideation by 1 to 3, which is the maximum score for each item and may mean an actual attempt. Similarly, Cunliffe & Cotterill [18] detected a relation between major stressful events and dermatological conditions and concluded that such a relation may increase suicidal behavior. Recently, Stanescu et al. [24] supposed the following one-direction way starting by psychological disorders associated with dermatological diseases leading to self-induced dermatological disorders due to psychiatric disorders, to major stressful events or psychic trauma, to severe chronic dermatological disorders and ending by suicidal ideation
The current study also detected a significant correlation between scores of the used inventories and duration and severity of vitiligo, patients’ BMI, gender and education. Similarly, Alharbi et al. [25] detected a higher frequency of moderate to severe depression among adolescents, single patients, those with lower than high school education and patients with shorter duration of the disease.
CONCLUSION
The results of the current study indicated a deleterious effect of vitiligo on patients’ psychological status. This is evident by the high percentage of participants who have mild-to-moderate depression. The effect of the disease on body image, especially the genital area, induced sexual dissatisfaction with an impact on sexual function.
RECOMMENDATION
Evaluation of the value of psychotherapy as a management regimen for vitiligo patients especially those with depression with special regard to the impact of vitiligo on QoL and sexual function.
LIMITATIONS
The study being limited to only one center and the lack of control groups needed to be overcome
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Research Ethics Committee at The Faculty of Medicine, Benha University, Egypt under approval no. 0044.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICTION
Informed consent was obtained from all the participants when they were enrolled.
AVAILABILITY OF DATA AND MATERIALS
The data and materials used to support the findings of this study are available from the corresponding author (G.A) upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author wished to thank Dr. Shereen M Abdel Wahab for her help in analysis of the responses of the questionnaires, Dr. Yusuf A Al-Kholy for preparing the online questionnaire and Via Translation Company [Registered at the Egyptian Translators & Linguists Association; Reg. No. 7148/2007 & Accreditation No. 1560] for preparing the Arabic versions of the used questionnaires. Also, the author wished to thanks to members of Dermatology Dep, Benha University Hospital for allowance to extract patients’ data out of the department registry.

