All published articles of this journal are available on ScienceDirect.

Localized Zosteriform bullous Pemphigoid on the Sites of a Healed Herpes Zoster: A Case Report and Literature Review
Abstract
Background:
Localized zosteriform bullous pemphigoid is a rare variant of bullous pemphigoid that is considered a manifestation of Wolf`s isotopic response. Only a few cases have been reported. We add another case to the body of knowledge in order to shed the light on this uncommon variant of bullous pemphigoid.
Case Report:
A 67-year old female patient developed vesiculobullous lesions at the sites of healed herpes zoster. The patient was diagnosed as a case of zosteriform bullous pemphigoid based on the clinical presentation and skin biopsy findings.
Conclusion:
Zosteriform bullous pemphigoid is a rare manifestation of Wolf`s isotopic response. A Skin biopsy must be performed early to ensure proper diagnosis and management.
1. INTRODUCTION
Wolf`s isotopic response is a dermatological phenomenon defined as the development of a new secondary skin disease at the site of a primary, often healed unrelated disease [1]. In most reported cases, the primary skin disease was herpes zoster [2]. Different skin disorders have been reported as a manifestation of this phenomenon, including lichen planus, lichen sclerosis et atrophicans, morphea, bullous pemphigoid, and others [2]. Localized bullous pemphigoid is a known yet rare variant of bullous pemphigoid that usually develops at sites of trauma, surgery, and radiation [3, 4]. Localized zosteriform bullous pemphigoid is another rare variant of the disease. Only a few cases of localized zosteriform bullous pemphigoid developing at sites of healed lesions of herpes zoster have been reported. Here, we report an additional case of this rare variant.
2. CASE REPORT
A 67-year-old female with a history of herpes zoster affecting the territory of the C-5 dermatome that was managed with systemic antivirals and had an uncomplicated course of treatment, resulting in crusting and eventual healing of the lesions.
Four weeks later, she started to develop new skin lesions at the site of the healed herpes zoster. The patient was given a trial of different topical agents but without any benefit, and she was referred for proper diagnosis. On clinical examination, the patient had erythematous, tense vesiculobullous, crusted skin lesions in a dermatomal distribution at the site of the healed herpes zoster lesions (Fig. 1).
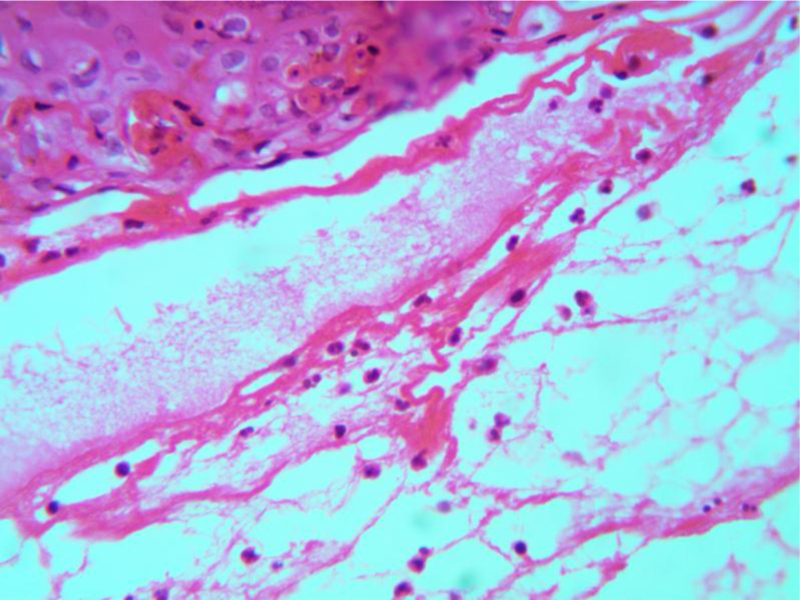
Skin biopsies were performed from lesional and perilesional skin and sent to for both routine histology and direct immunofluorescence study, respectively. Routine histopathological examination of hematoxylin and eosin-stained sections showed a subepidermal blister containing eosinophils and neutrophils, eosinophilic spongiosis, a mild superficial perivascular lymphoid cell inflammatory infiltrate containing eosinophils and neutrophils and papillary dermal edema; histologic findings that are consistent with bullous pemphigoid (Figs. 2 and 3).


A direct immunofluorescence study of perilesional, uninvolved skin showed linear deposition of IgG autoantibodies at the dermo-epidermal junction. An indirect immunofluorescence study was not performed. Accordingly, the diagnosis of localized zosteriform bullous pemphigoid was made. The patient was treated with prednisolone 0.5mg /kg/day and topical betamethasone valerate with excellent response and disappearance of the skin lesions after three months.
3. DISCUSSION
Bullous pemphigoid is the commonest immunobullous skin disease in the elderly, usually presenting as an itchy generalized vesiculobullous skin eruption [5]. The autoantibodies against bullous pemphigoid antigen 180(BP 180) and bullous pemphigoid antigen 230 (BP 230) are involved in the pathogenesis of bullous pemphigoid [6]. Bullous pemphigoid can be drug-induced [7]. The localized variant of bullous pemphigoid accounts for less than one-third of all cases of bullous pemphigoid and occurs at sites of trauma, surgery or radiation [4, 8]. Wolf`s isotopic response was recognized as a dermatological phenomenon with a precise definition in 1985 [9]. Wolf`s isotopic response can be defined as the development of new secondary skin disease at the sites of a healed unrelated primary skin condition [1, 9, 10] Various skin diseases have been reported to develop as a presentation of this phenomenon, including several neoplastic, inflammatory, infectious, granulomatous, and immunologic skin diseases [1]. The primary skin disease was herpes zoster in most of cases [2]. The time period between the healing of the primary disease and the appearance of the secondary is variable and can range from days to years [9]. Bullous pemphigoid is a rare manifestation of this phenomenon [2]. Localized zosteriform bullous pemphigoid is a rare variant of bullous pemphigoid. After reviewing the literature, only three other cases of localized zosteriform bullous pemphigoid have been reported to the best of our knowledge [11-13] (Table 1). All three cases were in elderly women. The duration between the healing of herpes zoster and the appearance of bullous pemphigoid was one month in two cases and six months in the other case. Our patient reported was also an elderly female who developed the vesiculobullous eruption four weeks after healing of the herpes zoster lesions.
| Case Number | Sex | Age | Involved Dermatomes | Time of Appearance after Herpes |
|---|---|---|---|---|
| 1 | Female | 79 years | T2-T4,C5,C6 | One month |
| 2 | Female | 80 years | T3 | Six months |
| 3 | Female | 87 years | C7-C8 | One month |
The exact mechanism for the development of this phenomenon is not known precisely, but different hypotheses have been suggested including, neural and immunologic causes [2, 10]. Persistent immune activation was investigated as a contributing factor for the development of this phenomenon [13, 10].
CONCLUSION
Localized zosteriform bullous pemphigoid is a manifestation of Wolf`s isotopic response; it should be considered in any patient with the vesiculobullous eruption at the sites of healed herpes zoster lesions. Skin biopsy is considered diagnostic and should not be delayed.
LIST OF ABBREVIATIONS
| IgG | = Immunoglobulin G |
| BP | = Bullous pemphigoid |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent has been obtained.
STANDARDS OF REPORTING
CARE guideline has been followed.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

