All published articles of this journal are available on ScienceDirect.

Hospital-based Dermatology Consultations in Jordan: A Cross-Sectional Study of Trends, Frequencies, and Health System Relevance
Authors Info & Affiliations
Abstract
Introduction
Skin diseases are a major global health issue and often require specialized hospital care. There is limited evidence on inpatient dermatology consultations in the Eastern Mediterranean Region, despite their importance to health systems and medical education.
Materials and Methods
A retrospective cross-sectional study was conducted at Jordan University Hospital from November 2022 to January 2024, reviewing 346 consultations to examine patient demographics, diagnoses, and treatments. The study also assessed referral patterns and the potential impact of these consultations on patient care, health systems, and medical staff training.
Results
Most referrals came from Internal Medicine (47.4%), Emergency Medicine (13.9%), and Surgery (13.3%). The most common diagnoses were inflammatory and immune diseases (39.0%) and infections (19.2%). Biopsies were the most commonly used diagnostic procedure (44.4%), and combination therapies, particularly those containing steroids and antihistamines, were the most common treatments.
Discussion
The study helps fill a regional evidence gap and highlights the important role of inpatient dermatology in supporting medical training and interdisciplinary inpatient care.
Conclusion
Dermatology consultations are important in inpatient care because they address common conditions like inflammatory and infectious diseases. They may contribute to improved patient outcomes and provide essential training for dermatology residents. Better education for non-dermatologist clinicians could encourage teamwork and further improve patient care.
1. INTRODUCTION
Skin disease is the fourth leading cause of nonfatal disease burden globally, with a high prevalence among hospitalized patients. In resource-poor settings, insufficient and timely dermatology input can delay diagnoses and treatment, worsening outcomes. Despite this, data from the Eastern Mediterranean region, particularly regarding inpatient dermatology consultation patterns, remain limited, representing a significant gap in the literature. This data is necessary for regional public health.
Although inpatient dermatology consultations have been described in several international settings, regional data from the Eastern Mediterranean region remain limited. This creates a knowledge gap regarding local referral patterns, disease burden, diagnostic practices, and treatment approaches in tertiary hospitals.
Skin disorders encompass a spectrum from minor to life-threatening conditions and often require specialized inpatient management [1-3]. Dermatologic consultations within hospitals are essential, as they address a wide range of conditions affecting patients across multiple departments [4, 5].
The primary aim of this study is to determine the total number of inpatient consultations performed by dermatologists at Jordan University Hospital (JUH), showing the importance of their presence in tertiary centers. The secondary aim is to assess consultation patterns, providing insights into prevalence, condition characteristics, chronicity, and diagnostic and treatment options. Additionally, the study highlights the educational value of inpatient consultations for residents, emphasizing opportunities to optimize care and strengthen collaboration between dermatologists and other specialists, supporting interdisciplinary collaboration within tertiary care settings [6-9].
In addition to characterizing consultation patterns, this study seeks to inform health system planning and workforce development by identifying priority dermatologic conditions and referral trends within a major tertiary hospital in Jordan.
This retrospective cross-sectional study, based on electronic medical record review, examined all inpatient dermatology consultations at JUH from November 2022 to January 2024 and analyzed patient demographics, diagnoses, consultation methods, and treatment approaches [10].
This study is among the few analyses of inpatient dermatology consultations in the Eastern Mediterranean Region, providing region-specific insights into referral patterns, disease distribution, and clinical practices in a tertiary care setting.
2. MATERIALS AND METHODS
This reA retrospective cross-sectional study was conducted at Jordan University Hospital, a tertiary referral center in Amman, Jordan, and included all inpatient dermatology consultations recorded between November 2022 and January 2024. The study included all inpatient dermatology consultations during this time. While the research was limited to one center, JUH is a referral hospital that sees a large and varied group of patients from across the country each day. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The manuscript was reviewed in accordance with the SAGER guidelines. Biological sex was collected as a demographic characteristic from electronic medical records and reported descriptively in the Results section. The study included all eligible patients regardless of sex and was not designed to evaluate sex-based differences in dermatological consultation patterns; therefore, sex-stratified analyses were not performed.
All inpatients who had a dermatology consultation during the study period were included. Patients were excluded if their medical records were incomplete or if their consultations were canceled without follow-up. Cases with incomplete or missing key variables were excluded from analysis. The proportion of excluded cases was minimal and unlikely to affect the overall findings significantly.
The IT department retrieved data from the hospital's electronic medical records. For each patient, we collected demographic details, including age and biological sex, primary diagnosis, admitting department, dermatological condition and its duration, diagnostic tests, and treatments. Treatment data were categorized by therapeutic class, but detailed information regarding dosage, route, frequency, and duration of treatment was not consistently available in the electronic medical records. It was therefore not included in the analysis. Patients were grouped according to these factors.
Dermatologic diagnoses were categorized into predefined groups (inflammatory/immune, infectious, drug-related) based on the clinical classification used in prior dermatology consultation studies.
Dermatologic diagnoses were categorized into predefined groups, including inflammatory/immune, infectious, drug-related, pregnancy-related, pigmentary, neoplastic/benign growth, trauma-related, genetic/congenital, vascular/lymphatic, hair/nail, metabolic/systemic, and other conditions. Categorization was based on clinical diagnosis documented in the medical record and commonly used groupings in inpatient dermatology consultation studies.
No formal sample size calculation was performed because this study employed a census sampling approach, including all eligible inpatient dermatology consultations recorded at Jordan University Hospital during the predefined study period (November 2022 to January 2024). As the study aimed to describe the complete population of consultations available within this timeframe rather than estimate outcomes from a selected sample, a sample size calculation was not required. The study period was selected based on the availability and completeness of electronic medical records during that period.
The proportion of excluded cases was minimal and considered unlikely to substantially influence the overall descriptive findings. However, this may introduce a small risk of selection bias.
The data analysis focused on determining the total number of consultations, the distribution of dermatological conditions across hospital departments, patterns in diagnosis and treatment, the impact of consultations on patient care, and training opportunities for dermatology residents and trainees. Given the study's descriptive objectives and the absence of predefined comparative hypotheses or standardized outcome variables, inferential statistical analyses were not performed. The primary aim was to characterize patterns of inpatient dermatology consultations rather than to evaluate statistically significant associations or causal relationships.
Data cleaning was performed in Microsoft Excel, descriptive analysis in Jamovi, and figures in Microsoft Power BI. We summarized the demographic and clinical characteristics of the study group using descriptive statistics. Continuous variables are shown as means (SD) and ranges [Min, Max], while categorical data are shown as frequencies and percentages.
Given the study's descriptive objectives and the absence of predefined comparative hypotheses, inferential statistical analyses were not performed. The primary aim was to characterize consultation patterns rather than assess causal or associative relationships.
This study was reviewed and approved by the University of Jordan (JUH) hospital Institutional Review Board (IRB) in Jordan and adhered to the tenets of the Declaration of Helsinki, ensuring ethical standards in design and ongoing monitoring. The approval number is: 29354.
3. RESULTS
During the study, a total of 346 patients were referred for inpatient dermatology consultations. The average age was 42.2 years (SD = 24.2), ranging from 1 month to 93 years. Of these patients, 55.5% were female, and 44.5% were male. Most referrals (68.6%) were for acute conditions, while 31.4% were for chronic conditions. On average, each patient had 1.88 visits (SD = 1.84) (Table 1).
Referrals were predominantly requested by the Internal Medicine department, accounting for 47.4% of cases (n = 164). Within Internal Medicine, hematology (26.8%), respiratory medicine (20.7%), and cardiology (11.0%) were the most frequently requested subspecialties for consultations. Emergency Medicine contributed 13.9% (n = 48) of referrals, while Surgery contributed 13.3% (n = 46). Within Surgery, the most common subspecialties were neurosurgery (30.4%), cardiothoracic surgery (15.2%), and orthopedic surgery (13.0%). Pediatrics also accounted for 13.3% (n = 46) of referrals, primarily from the respiratory (30.4%), neurology (19.6%), and endocrine (13.0%) subspecialties. Obstetrics and Gynecology contributed to 8.7% (n = 30) of referrals, while other specialties, including psychiatry and dentistry, accounted for 3.5% (n = 12) (Table 1) (Fig. 1a).
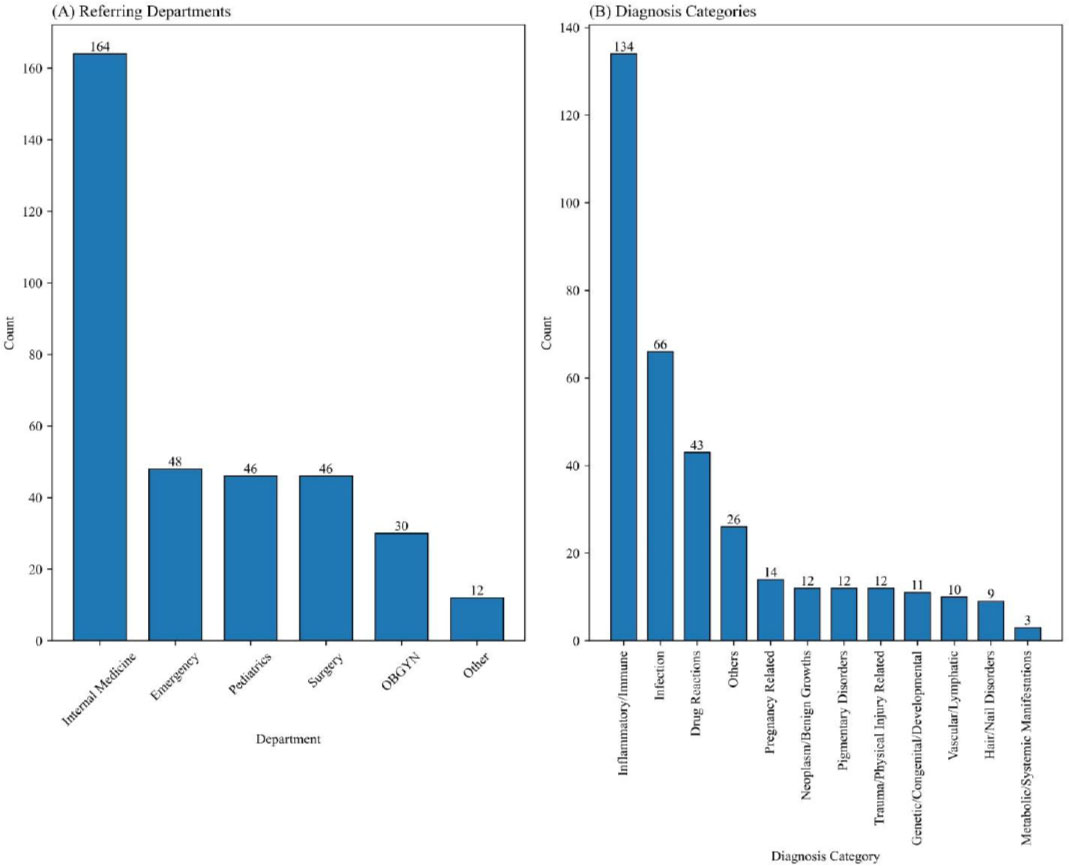
Inpatient dermatology referrals. (a) Distribution of referrals by Specialty. (b) Distribution of dermatologic disease categories.
| Variable | N (%) / Mean ± SD |
|---|---|
| Age, years | 42.2 ± 24.2 (range 0.08–93) |
| Gender | Female 191 (55.5), Male 153 (44.5) Note: Gender data were available for 344 patients; of these, 191 (55.5%) were female, and 153 (44.5%) were male. |
| Type of referral | Acute 236 (68.6), Chronic 108 (31.4) |
| Number of visits | 1.9 ± 1.8 (range 0–10) |
| Referral sources | |
| Internal Medicine | 164 (47.4) |
| Surgery | 46 (13.3) |
| Pediatrics | 46 (13.3) |
| Emergency Medicine | 48 (13.9) |
| Obstetrics & Gynecology | 30 (8.7) |
| Others | 12 (3.5) |
Among the 126 cases in which investigations were ordered, biopsies were the most common diagnostic procedure: 44.4% (n = 56) of patients had a biopsy ordered, and 52 underwent the procedure. Laboratory tests were performed in 27.0% (n = 34) of cases, and swab cultures were obtained in 22.2% (n = 28) of cases. Immunofluorescence was utilized in 9.5% (n = 12) of investigations. Other investigations, including blood, nasal, or nail cultures (3.2%), PCR (2.4%), Radioallergosorbent testing (1.6%), genetic testing (0.8%), and ultrasound (0.8%), were less frequently employed (Table 2).
| Variable | N (%) |
|---|---|
| Investigations (N = 126) | |
| Biopsy ordered/done | 56 (44.4) / 52 (41.3) |
| Laboratory tests | 34 (27.0) |
| Swab culture | 28 (22.2) |
| Immunofluorescence | 12 (9.5) |
| Other investigations* | 11 (8.7) |
| Treatments (N = 289) | |
| Combination therapy | 91 (31.5) |
| Steroids | 85 (29.4) |
| Antibiotics | 28 (9.7) |
| Antihistamines | 14 (4.8) |
| Antivirals | 10 (3.5) |
| Antifungals | 10 (3.5) |
| Emollients | 5 (1.7) |
| Other treatments | 46 (15.9) |
Combination therapy breakdown N (%): steroid+antihistamine: 31/91 (34.1%), steroid+emollient: 15/91 (16.5%), steroid+antibiotics: 14/91 (15.4%), antiviral+antibiotic: 10/91 (11.0%), steroid+antifungal: 5/91 (5.5%), steroid+antiviral: 2/91 (2.2%), antihistamine+emollient: 2/91 (2.2%), antibiotic+emollient: 1/91 (1.1%), ≥3 agents: 11/91 (12.1%).
Topical vs systemic distribution (N, % topical): steroids (45/85, 53% topical), antibiotics (16/28, 57% topical), antivirals and antifungals (8/10, 80% topical).
Referrals were classified into 11 main disease categories (Table 3). The most common category was inflammatory/immune diseases, comprising 134 cases (39.0%). Within this category, dermatitis accounted for 24.6% (n = 33), followed by vasculitis (19.4%, n = 26) and connective tissue / autoimmune disorders (12.7%, n = 17). Infections were the second most frequent category, constituting 19.2% (n = 66) of referrals. Among these, viral infections were the most prevalent (48.5%, n = 32), followed by bacterial (34.8%, n = 23) and fungal (16.7%, n = 11) infections. Drug reactions were identified in 43 cases (12.5%), with combination therapy reactions being the leading cause (34.9%, n = 15), followed by antibiotic reactions (25.6%, n = 11) and anticonvulsant reactions (11.6%, n = 5). Pregnancy-related conditions accounted for 4.1% (n = 14) of referrals, with pruritus of pregnancy as the most common (50.0%, n = 7). Pigmentary disorders accounted for 3.5% (n = 12), with post-inflammatory pigmentation disorder being the most frequent diagnosis (50.0%, n = 6). Referrals for neoplasms or benign growths constituted 3.5% (n = 12), with steatocystoma multiplex and nevus sebaceous contributing 25.0% (n = 3) and 16.7% (n = 2), respectively. Trauma-related conditions accounted for 3.2% (n = 11), while insect bites represented 36.4% (n = 4) of cases. Less frequent categories included genetic/congenital disorders (2.9%, n = 10), vascular/lymphatic conditions (2.6%, n = 9), hair/nail disorders (1.2%, n = 4), and metabolic/systemic diseases (0.9%, n = 3). Other diseases not categorized, including stria rubra and scabies infestations, accounted for 7.6% (n = 26) of cases (Fig. 1b).
| Disease Category | N (%) | Most Common Diagnoses | Most Common Referring Departments |
|---|---|---|---|
| Inflammatory / Immune | 134/346 (39.0) | Dermatitis 33/134 (24.6%), Vasculitis 26/134 (19.4%) | Internal Medicine 57/134 (42.7%), Emergency Medicine 24/48 (50.0%) |
| Infection | 66/346 (19.2) | Viral 32/66 (48.5%), Bacterial 23/66 (34.8%), Fungal 11/66 (16.7%) | Pediatrics 18/46 (39.1%), Internal Medicine 23/164 (14.0%) |
| Drug reaction | 43/346 (12.5) | Combination therapy 15/43 (34.9%), Antibiotics 11/43 (25.6%) | Internal Medicine 24/164 (14.6%), Surgery 8/46 (17.4%) |
| Pregnancy-related | 14/346 (4.1) | Pruritus of pregnancy 7/14 (50.0%) | Obstetrics and Gynecology 11/30 (36.7%) |
| Pigmentary disorders | 12/346 (3.5) | Post-inflammatory pigmentation 6/12 (50.0%) | – |
| Neoplasm / Benign growth | 12/346 (3.5) | Steatocystoma multiplex 3/12 (25.0%), Nevus sebaceous 2/12 (16.7%) | – |
| Trauma-related | 11/346 (3.2) | Insect bite 4/11 (36.4%) | – |
| Genetic / Congenital | 10/346 (2.9) | – | Pediatrics 6/46 (13.0%) |
| Vascular / Lymphatic | 9/346 (2.6) | – | – |
| Hair / Nail | 4/346 (1.2) | – | – |
| Metabolic / Systemic | 3/346 (0.9) | – | – |
| Other diseases | 26/346 (7.6) | e.g., stria rubra, scabies | – |
Of the 289 patients who received treatment, combination therapies were the most commonly prescribed (31.5%), with the most frequent combinations including steroid + antihistamine (34.1%) and steroid + emollient (16.5%). Steroid therapy alone was the second most common treatment (29.4%), with nearly equal distribution between topical (52.9%) and systemic (47.1%) use. Antibiotics alone were prescribed in 9.7% of cases, more often in topical formulations (57.1%) than in systemic formulations (42.9%). Less common treatments included antihistamines (4.8%), antivirals (3.5%), antifungals (3.5%), and emollients (1.7%) (Table 2).
When stratifying disease categories by specialty referral, the Internal Medicine department had referrals predominantly for inflammatory/immune conditions (42.7%), drug reactions (14.6%), and infections (14.0%). Emergency Medicine accounted for 48 referrals, with inflammatory/immune conditions being the most frequent (50.0%), followed by infections (18.8%). Inflammatory/immune conditions (34.8%) were the most common in Surgery, while Pediatrics primarily managed infections (39.1%) and inflammatory/immune conditions (26.1%). Obstetrics and Gynecology referrals (8.7%, n = 30) were primarily for pregnancy-related conditions (36.7%) and inflammatory/immune conditions (23.3%) (Table 3) (Fig. 2).
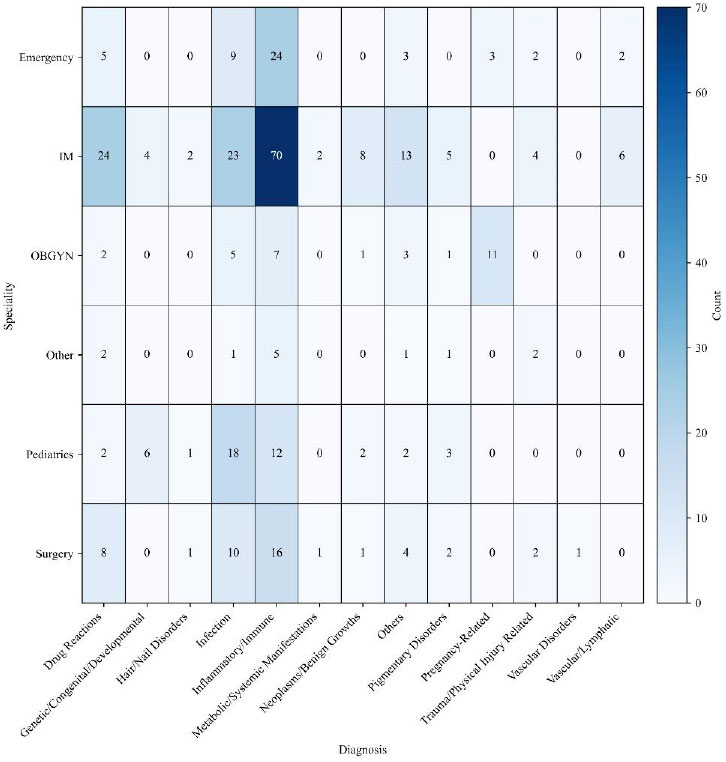
Distribution of dermatologic disease categories by referring department.
4. DISCUSSION
These findings provide new evidence from the Eastern Mediterranean region, where inpatient dermatology services remain insufficiently studied despite their significance to hospital resource utilization, quality of care, and medical education.
The predominance of inflammatory and immune diseases and infections emphasizes the importance of dermatology expertise within tertiary inpatient settings and supports targeted educational initiatives for non-dermatology clinicians.
Internal Medicine was the leading referring department, which is consistent with previous inpatient dermatology consultation studies [1, 4-6]. In the study, the leading surgical department that requested the most consultations was neurosurgery (30.4%), differing from Williams et al. (2016), who reported lower rates (2.9%). [6] Additionally, Pediatric referrals (13.3%) in the current study exceeded those reported by Mancusi & Festa Neto (2010) and Williams et al. (2016), which were 8% and 2.7%, respectively [2, 6].
In our study, biopsies were the most common diagnostic procedure, ordered in 44.4% of cases, and performed in 52 patients. This is similar to Alamri et al. (2022), who used biopsies as the most common diagnostic procedure, but with a much lower case frequency (10.0%). Laboratory tests were requested in 27.0% of cases in the present study, a proportion higher than the 6.0% reported by Alamri et al. Swab cultures were also more frequently used (22.2%) than in their findings (12.1%). Other investigations, including genetic testing and ultrasound, were rarely employed in both studies, indicating their limited role in dermatological consultations [4].
Inflammatory and immune diseases were the most common referral category in our cohort, consistent with prior inpatient dermatology studies from Brazil and India [6, 11].
Infections were also frequently encountered, consistent with prior inpatient dermatology consultation studies [2]. Drug reaction rates (12.5%) in our study were comparable to those reported by Fayne et al. (2020) in the U.S. and by Mancusi & Festa Neto (2010), at 14% and 8.9%, respectively [2, 12]. Pregnancy-related conditions (4.1%) and pigmentary disorders (3.5%) in our study were less frequently reported in comparable studies.
Combination therapies and topical steroids were among the most commonly prescribed treatments, similar to findings reported by Joseph et al. [1]. Additionally, antibiotics (9.7%) were prescribed more commonly as topical agents (57.1%) than as systemic agents in both studies, with topical antibiotics ranking second among the most commonly used drugs in Joseph et al. In comparison, less frequent treatments in our study included emollients (1.7%), which were among the most frequently used in Joseph et al. These findings suggest variation in treatment preferences across hospitals and countries, influenced by patient presentations and resource availability.
After stratifying disease categories referred by specialties for our study, the IM department predominantly referred cases related to inflammatory/immune conditions (42.7%), drug reactions (14.6%), and infections (14.0%), which is consistent with the findings of Williams et al. (2016), where consultations were commonly for fungal infections and eczematous dermatitis [6]. Moreover, Mancusi & Festa Neto (2010) showed that fungal infections and drug reactions were frequently consulted from IM [2].
The distribution of Emergency Medicine referrals differed from previous reports, potentially reflecting variations in patient populations, hospital settings, and referral practices. However, Rubegni et al.’s results showed that infections were the most common [13].
A study conducted in Germany by Hansen et al. found that the most common condition diagnosed via telemedicine for pediatric dermatological care was infection, a finding similar to ours. However, in our study, the patients were inpatients [7]. Data were missing from other studies.
Among surgical specialties, Inflammatory/immune conditions (34.8%) were the most common consultations, consistent with Williams et al. (2016), who reported generalized xerosis, intertrigo, eczematous dermatitis, and cutaneous fungal infections [6]. On the other hand, it is different from the results reported by Walia NS et al., which showed that sexually transmitted diseases and infections are the most common [14]. In both studies, Williams et al. and Lee J et al., neurosurgery's most common consultations were for drug rash. This could be due to anti-epileptic drugs being prescribed to this group of patients, inducing drug reactions [8].
Obstetrics and Gynecology referrals in our study (8.7%) were primarily for pregnancy-related conditions (36.7%) and inflammatory conditions (23.3%). In addition, Williams et al. reported that the most common consultations concerned infections and urticaria. In contrast, Walia et al. (2001) found that gynecological referrals often focused on vaginal discharge and pruritus vulvae [6, 14].
Our study results, supported by the literature, suggest that training non-dermatologists, the clinicians for the most common dermatologic conditions that present in their specialty, may support earlier recognition of common dermatologic conditions and strengthen interdisciplinary collaboration between specialties.
Some limitations must be acknowledged in our study. First, the study is limited by its retrospective design, which may introduce some information bias. For example, detailed treatment regimens, including medication dosages, administration frequency, and duration of therapy, were not consistently documented and therefore could not be analyzed. Second, the study was conducted at a single tertiary care center in the capital, where highly specialized consultants are available, which may limit the generalizability of the findings and make it challenging to apply the results to secondary or primary care centers. Third, the study did not evaluate clinical outcomes such as length of hospital stay, diagnostic modifications, treatment changes, or complications, limiting the ability to directly determine the overall clinical impact of dermatology consultations. Fourth, because inferential analyses and standardized inpatient outcome measures were not included, the findings should be interpreted as descriptive observations rather than evidence of statistically validated associations.
Despite the limitations, this study offers important insights into referral patterns and the educational significance of dermatology consultations in tertiary care settings. Enhanced collaboration between dermatologists and other specialties, facilitated by structured referral systems and targeted training programs, may have the potential to improve patient outcomes, minimize complications, and support regional health policy goals. The results highlight the public health importance of dermatology consultations as an integral component of comprehensive hospital care.
CONCLUSION
This study shows that dermatology consultations represent an important component in inpatient care at JUH and stresses the importance of having dermatologists available in tertiary care centers.
The findings showed that the most common referral category is inflammatory/immune diseases, followed by infections and drug reactions, highlighting the frequency of these conditions within inpatient consultations to address these conditions effectively. Consistent with the literature, Internal Medicine was the primary referring department, followed by Emergency Medicine and Surgery. These findings may help inform interdisciplinary educational initiatives. Dermatology consultations may support inpatient dermatologic care and interdisciplinary collaboration. Additionally, these consultations offer significant educational value by providing dermatology residents with essential training opportunities and supporting collaboration with other specialties.
The results point to the need for training programs to help non-dermatologist clinicians recognize common skin conditions in their fields and establish clear referral protocols. Such initiatives may support earlier recognition of common dermatologic conditions and improve communication between specialties.
The findings highlight the clinical and educational relevance of inpatient dermatology consultations within tertiary care settings. Future multicenter studies incorporating inferential analyses and patient outcome measures are needed to further evaluate specialty-specific referral patterns and the broader impact of inpatient dermatology services. Inpatient dermatology consultations may help improve care for individual patients in Jordan and the wider Eastern Mediterranean Region.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper with study conception and design, data collection, analysis and interpretation of results and draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| JUH | = Jordan University Hospital |
| STROBE | = Strengthening the Reporting of Observational Studies in Epidemiology |
| IRB | = Institutional Review Board |
| IM | = Internal Medicine |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Institutional Review Board (IRB) of Jordan University Hospital (JUH) reviewed and approved the study, Approval Number: 29354.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The requirement for written informed consent was waived by the IRB because this retrospective study involved review of existing anonymized electronic medical records, with no direct patient contact or intervention.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

