All published articles of this journal are available on ScienceDirect.

Psychological Characteristics of Children with Psoriasis
Authors Info & Affiliations
Abstract
Background:
The disease, regardless of its nosology, involves the child in a different deficient social situation. It creates two restraint conditions for the sick child: restriction of motions or restriction of cognitive activity. The interview with paediatric patients with psoriasis showed that 65% of them were stigmatised in the form of bullying, insults, and humiliation. Concerns about constant skin peeling and odour affect leisurely activity in 15-30% of children with psoriasis. This stigmatisation can lead to changes in behaviour, depression, anxiety, and apprehension. In adolescents with psoriasis, apprehension is increasingly mediated by the features of the attitude toward oneself and is of a contradictory, conflicting nature during this period. A persistently high anxiety level in childhood leads to a wide range of problems, the consequence of which can be impaired development of individual structures and functions and, ultimately, impaired formation of the personality structure as a whole.
Objective:
The article aims to determine the psychological characteristics of children with psoriasis aged 8–12 years.
Materials and Methods:
Characterological and behavioural traits were studied in 54 children with psoriasis aged 8–12 years using R. Cattell's multi-factor test (junior version). Characteristics of personality traits in terms of factor scoring were carried out by grouping them by communicative and emotional-volitional components.
Results:
It was determined that the majority of 8–12-year-old children with psoriasis have an average scoring of the basic factors by both communicative and emotional-volitional components. In addition, half of the children were found to have a low score of factor A “outgoingness” and factor Q3 “self-control”, while a third of the children had a low score of factors C “self-confidence” and F “risk proneness”. High scores were revealed for factors D “excitability” and O “apprehension”. The correlation analysis revealed a significant number of correlations between the bipolar factor indicators.
Conclusion:
The analysis using R. Cattell's Children's Personality Questionnaire identified the characteristic personality traits of children aged 8 to 12 years with psoriasis. The children are fairly adapted to society, showing activity and moderate sensitivity, and the ability to observe moral standards of behaviour. However, the disease's impact on the formation of psychological characteristics can already be traced: 50% of children with psoriasis have hyperexcitability and lack of self-control; one-third of patients have depressed moods, increased apprehension, seclusiveness, resentfulness, mistrustfulness and nervous tension, increased responsibility for their own actions and deeds, and lack of self-confidence; every fifth patient has a poor concentration of attention, fatigue and a simplified approach to problem-solving. The determined significant number of correlational pleiads between the bipolar factor scores in 8–12-year-old children with psoriasis allows designing approaches to individual and group psychocorrective and psychotherapeutic counselling.
1. INTRODUCTION
Psoriasis is a systemic chronic immune-mediated disease affecting mainly the skin and joints [1]. Psoriasis as a chronic dermatosis with obvious visible clinical manifestations, prolonged exacerbations, and poor response to treatment is a severe stress for the patient. Psoriasis has the same impact on the quality of a patient's life as diabetes, epilepsy, and atopic dermatitis [2].
In adult patients with psoriasis, different psychological features, as well as personality reactions to the disease, have been observed [3]. Using various questionnaires and psychological techniques, it has been concluded that adult patients are guilt-prone, have low frustration tolerance, and have passive behaviour proneness. They are anxious, emotionally unstable, vulnerable, dependent on others, secluded, and avoid society. They are also characterised by weak use of psychological defence mechanisms with a significant reduction in the indicators of “denial”, “substitution”, “repression”, and the phenomenon of alexithymia [4].
The disease, regardless of its nosology, involves the child in a different deficient social situation. It creates two restraint conditions for the sick child: restriction of motions or restriction of cognitive activity. The interview with paediatric patients with psoriasis showed that 65% of them were stigmatised in the form of bullying, insults, and humiliation. Concerns about constant skin peeling and odour affect leisurely activity in 15-30% of children with psoriasis [5]. This stigmatisation can lead to changes in behaviour, depression, anxiety, and apprehension. In adolescents with psoriasis, apprehension is increasingly mediated by the features of the attitude toward oneself and is of a contradictory, conflicting nature during this period. At the same time, apprehension itself exacerbates and intensifies this conflict – the resulting doubts about even real accomplishments further increase negative emotional experiences. Therefore, apprehension becomes fixed, acquires stable forms of realisation in behaviour, and becomes a personality trait with its own driving force [6]. A persistently high anxiety level in childhood leads to a wide range of problems, the consequence of which can be impaired development of individual structures and functions and, ultimately, impaired formation of the personality structure as a whole [7-9].
2. MATERIALS AND METHODS
Fifty-four children with psoriasis aged from 8 to 12 years were involved in the study: 30 females and 24 males. The average age of the children with psoriasis was 10 (9.0–11.0) years (Table 1). Treatment of children with psoriasis included external therapy and UVB therapy. The inclusion criteria for children were as follows: age 8–12 years, proven diagnosis of psoriasis, and possibility of regular monitoring. Exclusion criteria: under eight and over twelve years of age, other dermatologic diagnoses, the impossibility of regular monitoring. Characterological and behavioural personality traits were studied using R.B. Cattell's multi-factor test (junior version) [10]. Characteristics of personality traits of children aged 8–12 years with psoriasis in terms of factor scoring were conducted by grouping them by communicative and emotional-volitional components. The analysis was carried out taking into account the extreme and highest-rated scores.
The algorithm of this clinical study was approved by the Shupyk National Medical Academy of Postgraduate Education Ethics Commission (Protocol No. 4 dated 3 February 2020) as complying with the current legislation of Ukraine, modern ethical standards and principles of scientific clinical trials. The purpose of the study was explained to the parents of each child, and written consent was obtained to involve the child in the study.
The study materials were statistically processed using the StatTech v. 1.2.0 program (StatTech, Russia). The paired Student's t-test was used to compare groups by quantitative indicators for two linked samples. The direction and strength of the correlation between quantitative indicators were assessed using the Spearman's rank correlation coefficient. The correlation coefficient value (r) was interpreted by Chaddock's scale.
3. RESULTS
Based on Cattell's test estimated results, it was determined that the majority of children aged 8–12 with psoriasis have an average score of the basic factors (Table 2).
A separate assessment by factor B, measuring verbal intelligence, indicated that the greatest number of children (41/75.92%) with psoriasis had an average score of this factor. A low level for this factor was found in 10 (19.04%) subjects. Such factor scoring can be characterized by fatigue, reduced attention, simplified approach to problem-solving, which suggests the presence of emotional disorganization of thinking in these children. And only 3 children had a high score of the verbal intelligence indicator. These children have high intellectual abilities, a large amount of knowledge, and high learning capabilities.
Characteristics of the personality traits of 8–12-year-old children with psoriasis in terms of the communicative factors A, E, H, F scoring were as follows. For factor A “outgoingness”, the obtained results of the study demonstrate a nearly identical distribution of this factor between low and average scores in children with psoriasis. The low scores of the factor in 26 (48.15%) children were manifested with a shift in the balance towards lower sociability, seclusiveness, and insufficient flexibility in contacts. In addition, these children may have features of superficiality in interpersonal relationships, manifestations of resentfulness, mistrustfulness, egocentrism, and stubbornness. They are not interested in the lives of others, feel better alone, and prefer material things. Twenty-three (42.59%) children with an average score of the factor were normally sociable, according to their age.
Most children (36/66.67%) had average scores of factor E “self-assertiveness proneness”, which demonstrated a certain ability of children to adapt in the social environment. The number of children with low and high factor scores was almost the same, 10 and 8. Children with a low score on this factor (10/18.52%) lacked confidence in themselves, and their abilities were passive, careful, and friendly. Children with a high score of this factor (8/14.81%) were prone to leadership, stubbornness, and energetic, but could be rude, aggressive, and conflictive.
The majority of children with psoriasis (66.67%) were found to have an average score for factor F “risk proneness”, and almost a third of children (27.77%) had its low level. Children with the average scoring are risk-taking and able to realise the consequences of their own behaviour. Children with a lower score on this indicator are characterized by carefulness, enhanced responsibility, and excitation for their future and the consequences of their actions and deeds. They have a higher level of internal tension.
The score of “social boldness”, factor H, was average in the majority of children aged 8–12 years (46/85.18%), indicating a moderate expression of activity. It can be said that the characteristics of child-adult interaction and the child's desire for self-assertiveness will depend on the psychoemotional state of the adult with whom the child communicates, and in what circumstances this process occurs.
The analysis of the study data on the factors characterizing the communicative sphere showed that children with psoriasis have normative indicators of communicative sphere scoring. This indicates a sufficient level of adaptation to the social environment and activity. At the same time, children who have “peak” scores for the factors require attention. More than a third of the subjects showed features of introversion, seclusiveness, some resentfulness, and mistrustfulness. Almost a fifth of the patients showed fatigue, lack of attention concentration, and a simplified approach to problem-solving. It is supposed that these characteristics may be related to the child's disease, which in a certain way, affects the narrowing of their social circle.
The features of the emotional-volitional sphere in children with psoriasis were assessed according to factors C, D, G, I, O, Q3, and Q4.
Factor D “excitability” characterizes the child's ability to be balanced and control their volitional aspect in certain real-life situations. It should be noted that the greatest number of children with psoriasis (29/52.38%) had high scores for these factors. This indicates a lack of their self-control, concentration and attention, excessive manifestations of excitability and disruptive emotional reactions, even in minor situations or circumstances. Eighteen (33.33%) subjects with an average factor score had the ability to control their own behaviour, depended on their psychoemotional state and health status.
A fairly large number of children had a high score for factor O “apprehension”; the latter manifestations were considered the basis for the emergence of neuroticism. An upward bias of the factor balance was detected in 20 (37.03%) children. Such children have a lowered and depressed mood background, take their failures hard, and underestimate their own capabilities, knowledge, and abilities, depending on social influences and assessments of relevant persons. Among people, they behave modestly, feel uncomfortable, and keep themselves apart. Thirty-one children (57.40%) had average scores for factor O, which indicates an average level of apprehension in these children.
| Indicators | Me | Q1 – Q3 |
|---|---|---|
| Average age of children (years) | 10.00 | 9.00 – 11.00 |
| Average age at onset (years) | 9.00 | 6.00 – 9.75 |
| Average duration of disease (years) | 1.00 | 0.58 – 4.00 |
| Average duration of exacerbation (weeks) | 4.00 | 4.00 – 8.00 |
| Average PASI score at treatment initiation | 6.30 | 1.95 – 10.95 |
| Average PASI at the end of treatment | 0.00 | 0.00 – 0.60 |
| Average BSA | 17.70 | 6.70 – 29.55 |
| S.No. | Factor | Low | Average | High | ||||
| Quantity | % | Quantity | % | Quantity | % | |||
| 1 | A | Outgoingness | 26 | 48.15 | 23 | 42.59 | 5 | 9.26 |
| 2 | B | Verbal intelligence | 10 | 18.52 | 41 | 75.92 | 3 | 5.56 |
| 3 | C | Self-confidence | 15 | 27.78 | 34 | 62.96 | 5 | 9.26 |
| 4 | D | Excitability | 7 | 12.96 | 18 | 33.33 | 29 | 53.71 |
| 5 | E | Proneness to self-assertiveness | 10 | 18.52 | 36 | 66.67 | 8 | 14.81 |
| 6 | F | Risk proneness | 15 | 27.77 | 36 | 66.67 | 3 | 5.56 |
| 7 | G | Conscientiousness | 0 | 0 | 49 | 90.74 | 5 | 9.26 |
| 8 | H | Social boldness | 3 | 5.56 | 46 | 85.18 | 5 | 9.26 |
| 9 | I | Sensitivity | 3 | 5.56 | 43 | 79.63 | 8 | 14.81 |
| 10 | O | Apprehension | 3 | 5.56 | 31 | 57.40 | 20 | 37.04 |
| 11 | Q3 | Self-control | 28 | 51.85 | 26 | 48.15 | 0 | 0 |
| 12 | Q4 | Nervous tension | 3 | 5.56 | 36 | 66.67 | 15 | 27.77 |
A significant number of children with psoriasis (15/27.77%) were also revealed who had high scores for factor Q4 “nervous tension”, which described the general level of energetic excitability of the individual. These children are constantly in a state of excitement, find it difficult to calm down, feeling tired but unable to be inactive. They are characterized by emotional instability with a predominance of low mood, excitability, and sleep disturbance. Such children may have good intellectual abilities but poor academic performance. In 66.67% of children with psoriasis aged 8–12 years, an average formation level was detected by the factor indicating a balanced state of the indicator under study.
Factor C “self-confidence” in 34 (62.96%) children with psoriasis, was meanly expressed: children were able to be resilient, control their own psychoemotional state, and cope with life's obstacles. At the same time, 15 (27.78%) subjects showed a decrease in this indicator. This indicated manifestations of low self-esteem in children in case of failures, mood swings, lack of self-control of their own emotions, and dysadaptation. They may show resentfulness, often unjustified capriciousness, helplessness, fatigue, and troubled sleep. It can be stated that children with a pronounced low factor scoring predominantly had the psychoemotional state changeability, a lack of confidence in themselves and their abilities.
Factor G “conscientiousness,” in 49 (90.74%) subjects had average scores. Such a score indicated the balance of the indicator and the ability of individuals to comply with social rules and norms. In all likelihood, this factor in children may depend both on the social influence and on the child's individual characterological features.
As for factor I “sensitivity”, the majority of children – 43 (79.63%) patients – had an average score of the indicator, which was illustrative of a balance between the traits of “boldness” and “sensitivity”.
The factor Q3 “self-control” scores were divided almost equally between low and average ones. Twenty-eight (51.85%) of the 8–12-year-olds were found to have a low score of the factor. In children with psoriasis, this indicated a lack of self-discipline and control of their own behaviour. This is characterised by insufficient socialisation, lack of orderliness and constructiveness in activities. Children may show a lack of adaptation to life. At the same time, the average level of indicator formation was established in 26 (48.15%) children with psoriasis, indicating moderate self-control.
Consequently, most children with psoriasis aged 8–12 showed average self-control scores. In general, they are able to comply with generally accepted norms of behaviour and show moderate sensitivity. At the same time, more attention should be paid to children with extreme manifestations of the factors according to the technique applied. More than 50% of children with psoriasis had increased excitability and a lack of self-control. More than a third of patients were characterized by depressed mood and increased apprehension. Almost a third of those studied exhibited nervous tension, a lack of confidence in themselves and their own capabilities, and increased responsibility and understanding of the “causal relationships” of their own actions and deeds.
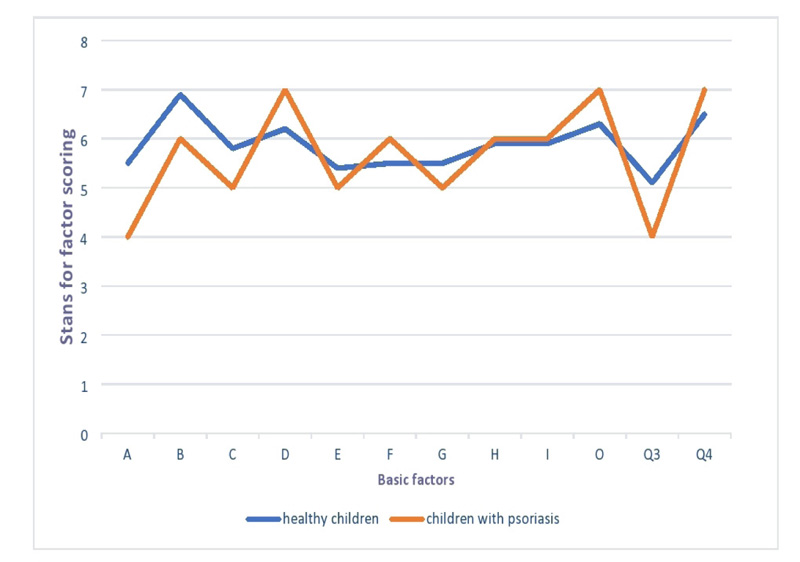
In general, the average scoring of almost all factors was observed in children aged from 8 to 12 years participating in the study. They have an average score for the following factors: В “verbal intelligence”, C “self-confidence”, E “proneness to self-assertiveness”, F “risk proneness”, G “conscientiousness”, H “social boldness”, I “sensitivity”. The average-low scores were identified for factor A “outgoingness,” and Q3 “self-control”. The average-high values were found for factor D “excitability”, O “apprehension” and Q4 “nervous tension”, which contributed to the peaks in the personality profiles of children with psoriasis for these factors (average values at the level of 7 stens), indicating a depressed mood with a sense of guilt, slight vulnerability and proneness to gloomy reflections. High ego tension can generate irritation (Fig. 1).
In assessing the influence and degree of influence of some personality characteristics on others by detecting correlation plaids between the bipolar factor scores [11], a significant number of correlations were found: insignificant, moderate, and significant. The assessment was made only for factors with relationship strength from 0.30 and statistically significant ones (p>0.05) (Fig. 2).
Factor A was found to correlate with factor B (r=0.350; p<0.001), indicating that manifestations of alienation, mistrustfulness and unsociability had been smoothened through increased intellectual activity. In addition, an increased factor A score will also give the child confidence (factor C (r=0.404; p<0.001)), conscientiousness (factor G (r=0.357; p<0.001)) and social boldness (factor H (r=0.393; p<0.001)), but will lead to decrease in factor D (r=-0.331; p<0.001), which will manifest as an increased lack of self-control, reduced concentration, the appearance of excitability and disruptive emotional reactions.
Factor C has a relationship with factors G (r=0.356; p<0.001) and H (r=0.510; p<0.001), showing that emotional maturity, restraint, and the ability to control the situation will increase conscientiousness and social boldness, but increased apprehension, sensitivity, underestimation of own capabilities, knowledge, and abilities will drive up resentfulness, mood variability and impaired adaptation in society, which the presence of inverse correlation with factors I (r=-0.431; p<0.001) and O (r=- 0.517; p<0.001) indicates.
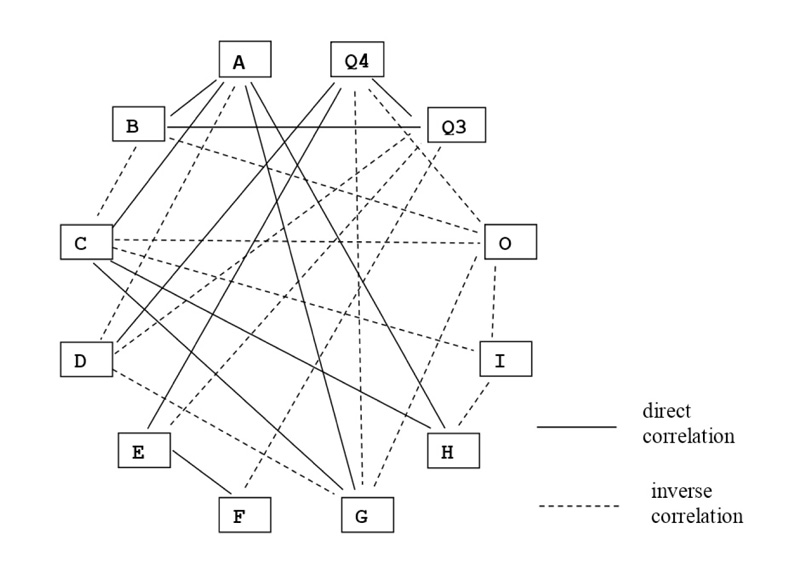
The factor D, which depends on the child's temperament characteristics and the upbringing conditions in the family, has an inverse correlation with factors G (r=-0.494; p<0.001) and Q3 (r=-0.383; p<0.001), and a direct correlation with factor Q4 (r=0.509; p<0.001). Increased excitability will lead to decreased conscientiousness and self-control and, at the same time, to increased nervous tension, excitability and sleep disturbance in children with psoriasis.
The direct correlation of factor E, demonstrating the child's ability to adapt to a social environment, with factors F (r=0.364; p<0.001), I (r=0.397; p<0.001), and Q4 (r=0.352; p<0.001) contributes to the children's awareness of the consequences of their own behaviour, the balance of male and female principles, but will lead to increased nervous tension, emotional instability, and excitability. Moreover, the presence of an inverse relationship with factor Q3 (r=-0,344; р<0,001) with an increased desire for self-assertion in the social environment may negatively affect the level of self-control in children with psoriasis, among whom 51.85% already have a low score of this factor. The factor G, which activates conscientiousness, normativity, and sense of duty, except for those listed above, found an inverse relationship with the other two factors: with factor O (r=-0.373; p<0.001) and factor Q4 (r=-0.586; p<0.001), and this leads to calming, normalization of mood, a real assessment of own abilities and capabilities.
There were revealed correlations between factor Q4 and O (r=0.500; p<0.001), Q4 and Q3 (r=-0.426; p<0.001), indicating increased development of the apprehension level, lack of self-confidence, decreased self-discipline and control of own behaviour with increased nervous tension in children with psoriasis.
Furthermore, the inverse relationship between factor B and factors O (r=-0.320; p<0.001) and C (r=-0.538; p<0.001), and a direct relationship with factor Q3 (r=-0.514; p<0.001) enables children with psoriasis to control their behaviour and assess the impact of their disease on shaping the opinions of others.
4. DISCUSSION
Determining the features of psychoemotional status is carried out for children with various diseases. For example, proneness to social avoidance, frustration, fatigue, and constant self-control was revealed in 17% of dental patients with chronic diseases of the oral mucosa [12]. Another study of adolescents with type 1 diabetes showed that they were prone to anxiety disorders (31.9%), behavioural disorders (19.1%), and mood disorders (14.3%) [13].
In dermatological patients, particularly those with atopic dermatitis, manifestations of trait anxiety, depression, low self-esteem, and autoaggression predominate. Patients cannot take care of themselves, cannot make decisions independently, and are waiting for care and decision-making from others. Patients with atopic dermatitis cannot analyse their needs and desires, and experience difficulties in self-expression and self-presentation. They have an inherent fear of making mistakes so as not to be rejected and unsuccessful [14].
Adult patients with psoriasis are characterised by hypochondriac and hysterical states, increased proneness to conflict [15], excessive vulnerability, mistrustfulness, suspiciousness, pessimistic assessment of outlook, misadaption of confidence and dependence system [16].
In our previous studies, while analysing the features of psychological status of adolescents with psoriasis using the R.B. Cattell's Multi-factor Personality Questionnaire (adolescent variant), it was found that in contrast to 8–12-yearold children with psoriasis, adolescents with psoriasis have a decrease in most bipolar factor scores: isolation (factor A “schizothymia”); compliancy and dependence on primary caregivers (E “obedience”); carefulness, vulnerability (F “desurgency”); hypersensitivity, timidity and narrowed social circle (H “shyness”); the importance of social approval and the need for group support (Q2 “degree of group dependency”); emotional instability, mood variability, increased excitability (C “degree of emotional stability”); slowness and some inertia (D “phlegmatism”); reduced normativity of behaviour (G “degree of moral standard acceptance”); practicability, pragmatism and cynicism (I “realism”); vigorousness, desire for social interaction with relatives (J “neurasthenia”); selfconfidence (O “self-confidence”); low volitional control (Q3 “degree of self-control”); lack of motivation and relaxation, which leads to laziness (Q4 “degree of internal tension”) (Table 3) [17].
Based on the data obtained, adolescents with psoriasis can be characterized as detached, reserved, careful, vulnerable, rigid, and obedient. They are dependent on primary caregivers and need group support; manifestations of criticism and avoidance of compromises balance with correctness in behaviour. They show slowness in action and certain pessimism. The narrowed social circle and some social passivity entail a desire for isolation and an individual style of activity. Adolescents with psoriasis are characterized by emotional and volitional features, such as sensitivity, emotional instability, mood swings, slowness, certain inertness, superficiality, and insufficient obligation. The manifestations of relaxation can lead to laziness and contribute to poor performance in activities or learning. In interpersonal relations, they are both sufficiently integrated into the process and cynical, impulsive, rigid, and somewhat self-confident, evoking hostility in others. They are able to actively respond to the satisfaction or dissatisfaction of personal needs, seek attention and social interaction, and are concerned about their own social status.
| S.No. | Factor | Low | Average | High | ||||
| Quantity | % | Quantity | % | Quantity | % | |||
| 1 | A | Schizothymia–afectothymia | 21 | 70.00 | 3 | 10 | 6 | 20.00 |
| 2 | B | Deception scale | 17 | 56.67 | 4 | 13.33 | 9 | 30.00 |
| 3 | C | Degree of emotional stability | 22 | 73.34 | 1 | 3.33 | 7 | 23.33 |
| 4 | D | Phlegmatism–excitability | 24 | 80.00 | 4 | 13.33 | 2 | 6.67 |
| 5 | E | Obedience–dominance | 26 | 86.67 | 3 | 10 | 1 | 3.33 |
| 6 | F | Desurgency–surgency | 28 | 93.33 | 2 | 6.67 | – | – |
| 7 | G | Degree of moral standards acceptance | 18 | 60.00 | 4 | 13.33 | 8 | 26.66 |
| 8 | H | Shyness–adventurism | 21 | 70.00 | 6 | 20 | 3 | 10.00 |
| 9 | I | Realism–sensitivity | 20 | 66.67 | 3 | 10 | 7 | 23.33 |
| 10 | J | Neurasthenia–Hamlet factor | 25 | 83.33 | 1 | 3.33 | 4 | 13.33 |
| 11 | O | Self-confidence–guilt proneness | 26 | 86.66 | 3 | 10 | 1 | 3.33 |
| 12 | Q2 | Degree of group dependency | 26 | 86.66 | 1 | 3.33 | 3 | 10.00 |
| 13 | Q3 | Degree of self-control | 25 | 83.33 | 3 | 10 | 2 | 6.67 |
| 14 | Q4 | Degree of internal tension | 27 | 90.00 | 1 | 3.33 | 2 | 6.67 |
In children with psoriasis aged 8–12 years, only 2 factors revealed the prevalence of low bipolar factor scores: Q3 (degree of self-control – 51.85%) and A (outgoingness – 48.15%). High scores for factor D (excitability) were found in more than half of the group of 8–12-year-old children with psoriasis (53.71%) and a third of children (37.04%) for factor O (apprehension). By other factors, most indicators have average scores.
CONCLUSION
The analysis using R. Cattell's Children's Personality Questionnaire identified the characteristic personality traits of children aged 8 to 12 years with psoriasis. In most cases, children with psoriasis aged 8–12 years are characterised by average expression of emotional-volitional and communication traits. The children are fairly adapted to society, showing activity, moderate sensitivity, and the ability to observe moral standards of behaviour. However, the disease's impact on the formation of psychological characteristics can already be traced: 50% of children with psoriasis have hyperexcitability and lack of self-control; one-third of patients have depressed moods, increased apprehension, seclusiveness, resentfulness, mistrustfulness, and nervous tension, increased responsibility for their own actions and deeds, and lack of self-confidence; every fifth patient has poor attention concentration, fatigue and a simplified approach to problem-solving.
The determined significant number of correlational Pleiades between the bipolar factor scores in 8–12-year-old children with psoriasis allows designing approaches to individual and group psychocorrective and psychotherapeutic counselling.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The algorithm of this clinical study was approved by the Shupyk National Medical Academy of Postgraduate Education Ethics Commission (Protocol No. 4 dated 3 February 2020) as complying with the current legislation of Ukraine, modern ethical standards, and principles of scientific clinical trials.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans were used in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Written consent was obtained to involve the child in the study.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

