All published articles of this journal are available on ScienceDirect.

Isolated Linear Discoid Lupus Erythematosus of Scalp Following Lines of Blaschko
Abstract
Discoid lupus erythematosus (DLE) is an inflammatory autoimmune disease leading to scarring and hair loss. Linear Discoid lupus erythematosus has been mentioned in the literature as a rare variant. This article describes isolated linear DLE of the scalp. We present a 26-year-old Saudi male who had unilateral linear DLE of the scalp with no involvement of other body sites and no systemic manifestations. This case is the first case of isolated linear DLE on the scalp. This presentation should be considered as a differential diagnosis of linear scarring alopecia as a distinct morphological pattern of DLE.
1. INTRODUCTION
Discoid Lupus Erythematosus (DLE) is considered the most common form of chronic cutaneous lupus erythematosus. Cicatricial alopecia is the end stage of this inflammatory disease when it affects the scalp. Clinically, DLE of the scalp typically shows erythematous papules or plaques and keratotic follicular plugging associated with pigmentary changes and atrophy of the skin. It has a female predominance, especially in the fourth and fifth generations [1].
Discoid Lupus Erythematosus is usually localized to the head and neck in 80% of the cases and it usually affects sun-exposed areas. If lesions develop beyond the head and neck area it is termed disseminated DLE. [2]. The risk of developing systemic lupus erythematosus in DLE patients is around 5-10%. Anti-nuclear antibodies can be seen in 20% of cases [3]. Cutaneous involvement of DLE along lines of Blaschko is quite rare [4]. We present a very rare case of Linear DLE of the Scalp in lines of Blaschko.
2. CASE REPORT
A 26-year-old Saudi male presented to the dermatology clinic with a 10-month history of a skin lesion on the left temple area with progressive hair loss. The lesion was asymptomatic with no itching or redness. The patient denied any trauma to the scalp.
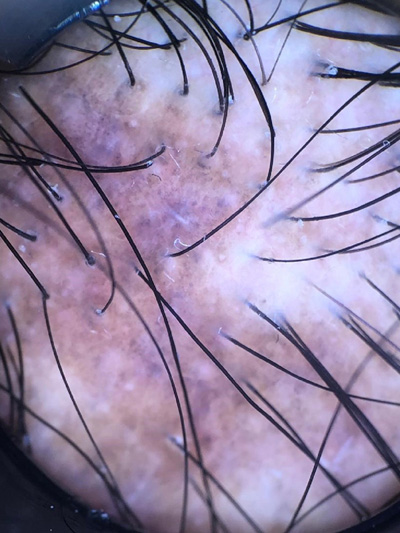
Physical examination showed a 1 × 12 cm unilateral linear well-defined pigmented plaque with atrophy, decreased hair density, perifollicular erythema and scaling over the superior border (Fig. 1A). There was no hair loss of the eyebrows, axillae, or groin area. The remaining skin, oral mucosa and nails were normal. He never complain of joint pain or photosensitivity and was otherwise healthy Dermoscopy showed areas of Perifollicular whitish halo, follicular keratotic plugs and telangiectasias (Fig. 1B) Antinuclear antibodies were negative.
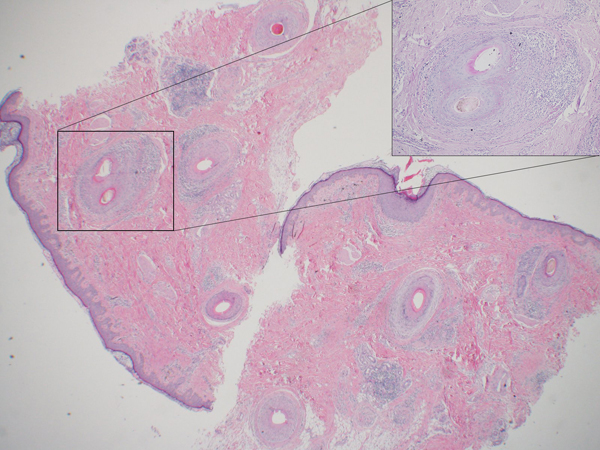
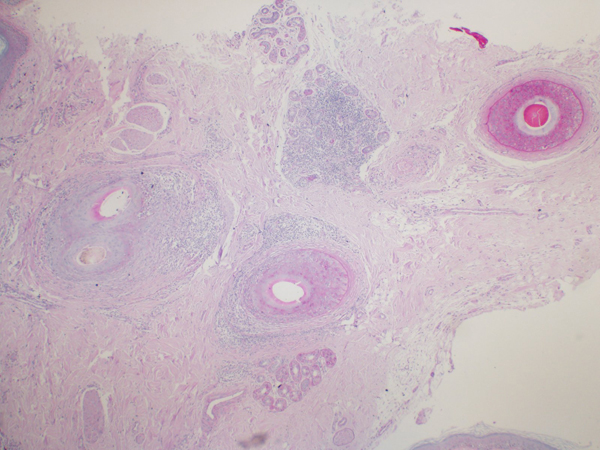
Skin biopsy taken from the erythematous area showed the eccrine gland and interfollicular lymphocytic infiltrate involving the upper follicular epithelium with dense perifollicular fibrosis, atrophic follicles, thick basement membrane and subepidermal pigment incontinence. (Figs. 2A, 2B).
A diagnosis of linear DLE of the scalp was made. The patient was prescribed clobetasol solution in combination with triamcinolone acetonide injections which were (1ml; 10 mg/mL) administered monthly. After 4 sessions, the lesions improved, hair regrowth noticed and no new lesions appeared.
3. DISCUSSION
Linear Cutaneous lupus erythematosus rarely reported, especially DLE of the scalp. We found only 2 case reports on isolated DLE affecting the scalp [2, 5]. However, linear DLE was reported more frequently in other sites like the face, neck and trunk. Linear cutaneous lupus in the literature was also observed in the form of tumid lupus, Subacute cutaneous lupus erythematosus, scleroderma overlapping cutaneous lupus and lupus panniculitis [6-8].

The patient did not have any history of trauma, and only one side of the scalp was affected. In contrast to this case, two similar case reports of linear DLE of the scalp had a facial extension [2, 5]. The patient had negative ANA and no other systemic manifestations of Lupus erythematosus as expected by majority with limited DLE [3].
Nevoid and Congenital skin diseases may follow lines of Blaschko. However, an inflammatory skin condition rarely has such a presentation [8]. Happle argued that in polygenic diseases, superimposed segmental manifestation should be used rather than segmental mosaicism. Type 1 or 2 segmental mosaicism is only applicable to monogenic inherited diseases or traits [9].
Lichen Planopilaris (LPP) should be considered as a differential diagnosis in this case. Differentiating DLE from LPP can be difficult as overlapping features occur clinically as well on pathology samples [10]. Clinical features favoring DLE include follicular plugging, depigmented or hypopigmented areas of skin and hyperpigmented surroundings. Although, histology of DLE may have perifollicular inflammation as seen in LPP, marked interstitial and perivascular inflammatory infiltration is often seen. Furthermore, thickening of the basement membrane and mucin deposition is observed [1, 3, 10].
The patient has liner DLE lesions involving only the scalp, making this the first case report presenting with isolated linear DLE exclusively on the scalp. We think that his lesions follow the lines of Blaschko. Unilateral affection and the absence of any trauma history make Kobnerization less likely. Linear DLE of the scalp should be considered as a differential diagnosis of linear scarring alopecia. This may be a distinct morphological pattern of DLE.
CONCLUSION
The first case of isolated linear DLE of the scalp is reported in this paper. When addressing linear scarring alopecia, linear DLE of the scalp must be recognized as a unique entity.
ETHICS APPROVAL AND CONSENT TO PARTIIPATE
This study was approved by the IRB (Institutional Review Board) (PSAU/COM/RC/IRB/A/35).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Each participant signed an informed consent to participate in the study.
STANDARD OF REPORTING
CARE guidelines and methodology were followed to conduct the study.
FUNDING
None
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

